PSYCHIATRIC NURSING NOTES by Ana Francisca C. Viado, R.N.
DEFINITION: INTERPERSONAL PROCESS WHEREBY THE PROFESSIONAL NURSE ASSIST THE INDIVIDUAL, THE FAMILY, & THE COMMUNITY TO PROMOTE MENTAL HEALTH, PREVENT MENTAL ILLNESS, & FIND MEANING IN ITS EXPERIENCE.
WHAT IS ESSENTIAL IN PSYCHIATRIC NURSING? THERAPEUTIC RELATIONSHIP.
THERAPEUTIC RELATIONSHIP is a client-centered relationship which focuses on the clients thoughts & ideas, feelings, and experience.
ELEMENTS:
1. Trust & Congruency
2. Acceptance
3. Genuine Interest
4. Positive Regard
5. Empathy
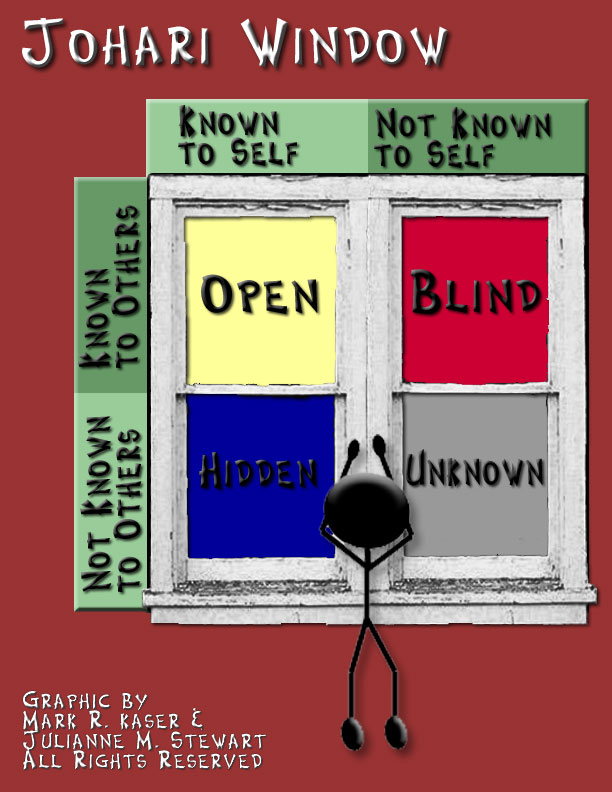
6. Self-awareness
THERAPEUTIC USE OF SELF: is the ability of the nurse to sustain and maintain a therapeutic relationship with the client.
PHASES OF THERAPEUTIC RELATIONSHIP
1. PRE-INTERACTION PHASE: In this phase of therapeutic relationship there is no initial meeting between the nurse and the client. The nurse will do the following activities: SELF AWARENESS and REVIEW OF MEDICAL RECORDS.
2. ORIENTATION PHASE: This is the initial meeting between the nurse and the client. The goal in this phase of therapeutic relationship is to ESTABLISH RAPPORT & TO DEVELOP TRUST. The nurse sets contracts which then includes the duration of the relationship ergo the nurse is already introducing TERMINATION phase with the client.

3. WORKING PHASE: The longest phase which includes majority of the Nurse-Patient-Interaction. In this phase, the nurse prepares the client for termination by reminding the client how long the relationship has already been existing and how long the remaining days is gonna be.

4. TERMINATION PHASE: End of the relationship. The nurse evaluates the client if goals are met.

MENTAL HEALTH & MENTAL ILLNESS
MENTAL HEALTHis formerly defined as the absence of mental illness. Today we consider it as the overall emotional and psychological state of an individual which possess the following qualities:
1. Autonomy & Independence.
2. Self-awareness.
3. Stress Management.
4. Self-actualization.
5. Interpersonal Skills.
6. Mastery of the environment.
7. Reality Orientation.
MENTAL ILLNESS. Any disease affecting the brain that influence the way a person thinks, feels, behave, & realate to others and environment which causes impairment in functioning.

MOOD DISORDERS
CHARACTERIZED BY EXTREME SADNESS/ELATION OR FLUCTUATING FEELINGS OF MILD TO EXTREME PERIODS OF EXTREME HAPPINESS TO EXTREME SADNESS. I.E. DEPRESSION, BIPOLAR DISORDERS
DEPRESSION
is common among women than men but the incidence decreases with age among women and incidence of depression increases with age in men. Characterized by Hopelessness, Helplessness, and Worthlessness.
A DEPRESSED PERSON has......
Sleep pattern either increased or decreased
Appetite either increased or decreased
Diminished drive or motivation: AVOLITION
Diminished pleasure: ANHEDONIA
Decreased concentration
Psychomotor Agitation
Psychomotor Retardation
Suicidal Thoughts
Major Depressive Disorder
Presence of 3 or more symptoms present for at least two weeks.
Dysthymic Disorder
Presence of 2 to 3 symptoms present for 2 years

MANAGEMENT:
1. Ensure a safe environment. Institute suicide precautions.
2. Established a therapeutic environment
> spend a non-demanding time with the client. (OFFER ONESELF)
> promote expression of feelings (ACTIVE LISTENING)
3. Increase client's self-esteem by engaging the client in activities that would ensure success.
1. Ensure a safe environment. Institute suicide precautions.
2. Established a therapeutic environment
> spend a non-demanding time with the client. (OFFER ONESELF)
> promote expression of feelings (ACTIVE LISTENING)
3. Increase client's self-esteem by engaging the client in activities that would ensure success.
BIPOLAR DISORDER
involves extreme mood swings from episodes of mania to episodes of depression.
BIPOLAR I: alternation between MANIA & EUTHYMIA
BIPOLAR II: alternation between DEPRESSION & EUTHYMIA
MANIC-DEPRESSIVE: cycles alternate between periods of DEPRESSION back to NORMAL then to MANIA seen in 2 weeks interval.
CYCLOTHYMIC: MANIC-HYPERACTIVE-DEPRESSED-HYPOACTIVE seen in 2 years interval
BIPOLAR I: alternation between MANIA & EUTHYMIA
BIPOLAR II: alternation between DEPRESSION & EUTHYMIA
MANIC-DEPRESSIVE: cycles alternate between periods of DEPRESSION back to NORMAL then to MANIA seen in 2 weeks interval.
CYCLOTHYMIC: MANIC-HYPERACTIVE-DEPRESSED-HYPOACTIVE seen in 2 years interval

MANIC
MOOD: elavated, euphoric. Usually this client would use BRIGHTLY COLORED CLOTHES.
SPEECH: pressured, loud, & rapid
Flight of ideas could lead to poor judgment which predisposes the client to injury.
HYPERACTIVITY could lead to physical exhaustion
GRANDIOSITY & FALSE SENSE WELL-BEING. Remember all behavior has meaning which could mean that there is an underlying anxiety.
DEFENSE MECHANISM: Denial & Reaction Formation
MANAGEMENT:
Maintain safety- set realistic limits
Allow freedom of expression
Nurses do not cut-off manic stream
Involve client in activities that do not require concentration
Help client recognize & express anxiety.
** History of these clients would reveal that he has not eaten or slept for days already. What to do?
1. Offer FINGER FOODS or ON-THE-GO foods. (High in CALORIES)
2. Promote SLEEP by
> creating a restful environment
> establishing a bedtime routine (TSB, MASSAGE, MUSIC)
SPEECH: pressured, loud, & rapid
Flight of ideas could lead to poor judgment which predisposes the client to injury.
HYPERACTIVITY could lead to physical exhaustion
GRANDIOSITY & FALSE SENSE WELL-BEING. Remember all behavior has meaning which could mean that there is an underlying anxiety.
DEFENSE MECHANISM: Denial & Reaction Formation
MANAGEMENT:
Maintain safety- set realistic limits
Allow freedom of expression
Nurses do not cut-off manic stream
Involve client in activities that do not require concentration
Help client recognize & express anxiety.
** History of these clients would reveal that he has not eaten or slept for days already. What to do?
1. Offer FINGER FOODS or ON-THE-GO foods. (High in CALORIES)
2. Promote SLEEP by
> creating a restful environment
> establishing a bedtime routine (TSB, MASSAGE, MUSIC)
SUICIDE
intentional act of killing oneself.
SUICIDE IDEATION: ideas/thoughts of suicide which can be active(plans & action) or passive(plans)
SUICIDE ATTEMPT: failed/incomplete suicide act
WHO ARE CONSIDERED SUICIDAL?
Sex: more common in MALE
Age: seen mostly in adolescents, also seen in early & late adulthood.
Depression
Previous attempt: has to be observed for a period of 2 years most critical of which are the FIRST # MONTHS
Unemployed
Family history
Serious disease
SUICIDE IDEATION: ideas/thoughts of suicide which can be active(plans & action) or passive(plans)
SUICIDE ATTEMPT: failed/incomplete suicide act
WHO ARE CONSIDERED SUICIDAL?
Sex: more common in MALE
Age: seen mostly in adolescents, also seen in early & late adulthood.
Depression
Previous attempt: has to be observed for a period of 2 years most critical of which are the FIRST # MONTHS
Unemployed
Family history
Serious disease

FATALITY RATE OF SUICIDE METHODS:
1. Use of a gun 85% FATAL
2. Suffocation 69% FATAL
3. Fall 31 % FATAL
4. Poisoning/overdose 2% FATAL
5. Cut/Pierce 1% FATALSource: Vyrostek SB, Annest JL, Ryan GW. Surveillance for fatal and nonfatal injuries--United States, 2001. MMWR. 2004:53(SS07);1-57. http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5307a1.htm
SUICIDE PRECAUTIONS:
1. Provide a SAFE environment
1.1 STAY with the client
LOW LETHALITY POTENTIAL: provide unrescheduled monitoring not exceeding 10 minutes interval
HIGH LETHALITY POTENTIAL: one on one direct supervision without exemption, nurse must be 2-3
feet away from the client
1.2 REMOVE all harmful objects
2. ASSESS the client: ask DIRECT QUESTIONS
3. INFORM the members of the health team about the planned suicide act.
4. Set a NO-SUICIDE contract.
5. Observe for the impending signs of suicide:
Sudden cheerfulness
Giving away of prized possession
Suicide note
Request for a family visit one last time
Verbalization of extreme hopelessness
6. Document all assessment & intervention done
2. Suffocation 69% FATAL
3. Fall 31 % FATAL
4. Poisoning/overdose 2% FATAL
5. Cut/Pierce 1% FATALSource: Vyrostek SB, Annest JL, Ryan GW. Surveillance for fatal and nonfatal injuries--United States, 2001. MMWR. 2004:53(SS07);1-57. http://www.cdc.gov/mmwr/preview/mmwrhtml/ss5307a1.htm
SUICIDE PRECAUTIONS:
1. Provide a SAFE environment
1.1 STAY with the client
LOW LETHALITY POTENTIAL: provide unrescheduled monitoring not exceeding 10 minutes interval
HIGH LETHALITY POTENTIAL: one on one direct supervision without exemption, nurse must be 2-3
feet away from the client
1.2 REMOVE all harmful objects
2. ASSESS the client: ask DIRECT QUESTIONS
3. INFORM the members of the health team about the planned suicide act.
4. Set a NO-SUICIDE contract.
5. Observe for the impending signs of suicide:
Sudden cheerfulness
Giving away of prized possession
Suicide note
Request for a family visit one last time
Verbalization of extreme hopelessness
6. Document all assessment & intervention done
THOUGHT DISORDERS
characterized by distorted thinking & sensory perception.
SCHIZOPHRENIA clients with this disorder has problems on the following areas:
1. Speech Pattern:
clang association: "Jill went up the hill to pay the bill and kill bill"
neologism: "bekbay vorbi bibay"
verbigeration: "ako si m16 ratatatatatatatatata"
echolalia: "goodmorning mang pedro" "goodmorning mang pedro"
word salad: fruit. table. chek. battery.
2. Affect: flat, blunt, inappropriate
3. Perception: Hallucination, Illusion, Delusion
4. Occupation Functioning
5. Thought content
FLIGHT OF IDEAS: I hate mondays. Oh rain please go away. I love Karla.
LOOSE ASSOCIATION: disturbance of thinking in which ideas and thoughts
becomes vague and fragmented
SCHIZOPHRENIA clients with this disorder has problems on the following areas:
1. Speech Pattern:
clang association: "Jill went up the hill to pay the bill and kill bill"
neologism: "bekbay vorbi bibay"
verbigeration: "ako si m16 ratatatatatatatatata"
echolalia: "goodmorning mang pedro" "goodmorning mang pedro"
word salad: fruit. table. chek. battery.
2. Affect: flat, blunt, inappropriate
3. Perception: Hallucination, Illusion, Delusion
4. Occupation Functioning
5. Thought content
FLIGHT OF IDEAS: I hate mondays. Oh rain please go away. I love Karla.
LOOSE ASSOCIATION: disturbance of thinking in which ideas and thoughts
becomes vague and fragmented

AGE OF ONSET: MALE- 15-25 years of age
FEMALE- 25-35 years of age
CAUSE: MULTIFACTORIAL
1. HEREDITARY
SINGLE PARENT- 15 %
BOTH PARENTS- 35 %
TWINS- IDENTICAL 50 %
FRATERNAL 15 %
2. ENVIRONMENT- Poverty
3. NEUROCHEMICAL- Increased Dopamine
Increased Serotonin
SUBTYPES:
1. PARANOID: preoccupation with one or more delusions & frequent auditory hallucination
hostile & aggressive
2. DISORGANIZED/HEBEPHRENIC: inappropriate or flat affect
disorganized speech or behavior
loose association
3. CATATONIC: marked psychomotor disturbance
CATATONIC STUPOR: MOTIONLESS (waxy flexibility, mutism, negativism)
CATATONIC EXCITEMENT: EXCESSIVE MOTOR ACTIVITY (echolalia, echophraxia)
4. UNDIFFERENTIATED: mixed schizophrenic symptoms but do not meet the criteria for paranoid, disorganized, and catatonic.
5. RESIDUAL: characteristic symptoms are no longer present.
FEMALE- 25-35 years of age
CAUSE: MULTIFACTORIAL
1. HEREDITARY
SINGLE PARENT- 15 %
BOTH PARENTS- 35 %
TWINS- IDENTICAL 50 %
FRATERNAL 15 %
2. ENVIRONMENT- Poverty
3. NEUROCHEMICAL- Increased Dopamine
Increased Serotonin
SUBTYPES:
1. PARANOID: preoccupation with one or more delusions & frequent auditory hallucination
hostile & aggressive
2. DISORGANIZED/HEBEPHRENIC: inappropriate or flat affect
disorganized speech or behavior
loose association
3. CATATONIC: marked psychomotor disturbance
CATATONIC STUPOR: MOTIONLESS (waxy flexibility, mutism, negativism)
CATATONIC EXCITEMENT: EXCESSIVE MOTOR ACTIVITY (echolalia, echophraxia)
4. UNDIFFERENTIATED: mixed schizophrenic symptoms but do not meet the criteria for paranoid, disorganized, and catatonic.
5. RESIDUAL: characteristic symptoms are no longer present.
CLASSIFICATION ACCORDING TO SYMPTOMS
POSITIVE
KEYWORD: EXCESS in behavior
Ambivalence
Associative looseness
Flight of ideas
Echophraxia
Delusions
Hallucinations
Illussion
Ambivalence
Associative looseness
Flight of ideas
Echophraxia
Delusions
Hallucinations
Illussion
NEGATIVE
KEYWORD: DEFICITS in behavior
Alogia (poverty of speech)
Anhedonia (lack of pleasure)
Apathy (state of indifference)
Avolition (lack of drive or motivation)
Affect is blunt/flat
Alogia (poverty of speech)
Anhedonia (lack of pleasure)
Apathy (state of indifference)
Avolition (lack of drive or motivation)
Affect is blunt/flat
NURSING CARE
1. Establish a therapeutic environment: safe, non-threatening environment
2. Develop trust. Be consistent in keeping appointments.
3. Encourage verbalization but do not cross-examine the client.
4. Initiate interaction.
5. Present reality and acknowledge experience
6. Recognize & support clients accomplishment
7. Assist in ADL
8. Attitude therapy
Paranoid: Passive-Friendliness, must maintain physical boundary: 3-4 feet
Alone/withdrawn: Active-Friendliness
Manipulative: Matter-of-fact approach
Disorganized: no Demand attitude
Depressed: Kind Firmness
2. Develop trust. Be consistent in keeping appointments.
3. Encourage verbalization but do not cross-examine the client.
4. Initiate interaction.
5. Present reality and acknowledge experience
6. Recognize & support clients accomplishment
7. Assist in ADL
8. Attitude therapy
Paranoid: Passive-Friendliness, must maintain physical boundary: 3-4 feet
Alone/withdrawn: Active-Friendliness
Manipulative: Matter-of-fact approach
Disorganized: no Demand attitude
Depressed: Kind Firmness
ANXIETY DISORDERS
Characterized by a response of excessive or uncontrollable fear, anxiety, or nervousness to certain situations or objects.
ANXIETY a vague feeling of dread or apprehension caused by anticipation of danger.
LEVELS OF ANXIETY
MILD: widened perceptual field
client becomes ALERT
with logical reasoning & problem solving skills (OPTIMAL LEARNING LEVEL)
slight muscle tension
preparation of body for constructive action
MODERATE: perceptual field is narrowed to immediate task
client becomes selectively attentive
problem solving & reasoning skills with effort & assistance
moderate muscle tension
increase vital signs & slight muscle tension
preparation of body for protective action
SEVERE: perceptual field is reduced to one detail or scattered details
problem solving & reasoning skills is ineffective (DISORIENTATION)
poor eye contact
loud & rapid speech
severe muscle tension
preparation of body for fight or flight
PANIC: perceptual field reduced to self
client is irrational
feeling overwhelmed & out of control
depletion of body resources
actual fight or flight
last 5-30 minutes
NURSING INTERVENTION: nurse must be aware of his/her own level of anxiety
1. Assess level of anxiety
MILD: provide health teaching
MODERATE: use short, simple sentences
speak slowly to ensure client is taking in information correctly
SEVERE: care is directed to lower the client's anxiety level
stay with the client
speak in a low, calm, & soothing voice
if client is restless, walk with the client while talking
deep breathing exercises
PANIC: primary concern is to ensure SAFETY
stay with the client
the nurse must keep talking to the client in a comforting manner
provide a small, quiet, non-stimulating environment
ANXIETY DISORDERS
1. Generalized Anxiety Disorder
Characterized by at least 6 months of persistent & excessive worry & anxiety
Most common anxiety disorder
Presence of 3 or more of the following evidences of anxiety:
1. Reduce anxiety: develop trust, promote acceptance & convey empathy
encourage verbalization
2. Assist patient in examining problem solving methods
2. Panic Disorder
recurrent panic attacks & are worried about having more attacks
fear of losing control, feeling of going crazy, having heart attacks, and or dying
associated with agoraphobia
DURATION: 30 minutes to 1 Hour PEAK: 10 minutes
NSG CARE:
1. Promotes safety measures & comfort
3. Provide relaxation exercises
4. Engage client to explore how to lessen stressors & anxiety provoking situations
3. Obsessive-Compulsive Disorder
OBSESSION: refers to the recurrent & persistent thoughts/ideas/impulses COMPULSION: refers to the repetitive & ritualistic actions/behavior
ergo when we say OBSESSIVE-COMPULSIVE disorder the client is having a persistent & recurrent thoughts/impulse that consumes the person therefore leading to anxiety. In order for the client to neutralize the anxiety the client has to do things over and over again that interferes with the clients activities of daily living.
NSG CARE:
1. Encourage the client to talk about feelings/obsessions/rituals
2. Gradually lessen the time for the client to carry out ritualistic behavior
3. Encourage the client to use techniques to manage anxiety
4. Assist client to complete daily routine & activities
4. PHOBIC DISORDER
intense irrational fear of an external object, activity or situations.
NSG CARE:
1. Non-critical attitude
2. Provide safety & comfort measures
3. Help patient recognize that their behavior is a method of avoiding anxiety
4. Behavior Therapy
5. DISSOCIATIVE DISORDER
group of mental disorder that affects a client's consciousness, memory, identity, or environmental perception.
DEFENSE MECHANISM: DISSOCIATION. Helps a person protect the emotional self from recognizing the full effect of a traumatic event by allowing the mind to forget or remove itself from the painful memory.
TRAUMATIC EVENT --> FEAR/HORROR --> DISSOCIATIOVE SYMPTOMS (DURING/IMMEDIATELY AFTER EVENT)
DISSOCIATIVE AMNESIA: Loss of memory
DISSOCIATIVE FUGUE: Escape!
DEPERSONALIZATION: Client is detach from mental process or body
DISSOCIATIVE IDENTITY D/O: 2 or more distinct identities that
recurrently take control of behavior accompanied by inability to recall
personal information.
NSG CARE:
1. Institute safety measures
2. Establish a therapeutic environment
3. Relaxation technique
4. Use positive distractions: Physical exercise
Music
Talking to others
Recreational activity
5. Promote self-esteem: view client as a survivor of trauma rather than a victim
6. POST-TRAUMATIC STRESS DISORDER
A disorder that develops after an exposure to a clearly identifiable trauma that threatens self, others, & sense of control or hope.
TRAUMATIC EVENT --> FEAR/HORROR --DISSOCIATIVE SYMPTOMS --> FLASHBACK --> SLEEP DIFFICULTY
HYPER VIGILANCE
IRRITABILITY
↓
AVOIDANCE OF STIMULI R/T TRAUMA
↓
IMPAIRMENT IN FUNCTIONING
ONSET: ACUTE within 6 months after event
DELAYED 6 months & more
DURATION: ACUTE 1-3 months
CHRONIC 3 months & more
GOAL OF NSG CARE: Develop TRUST
1. Non-judgmental & honest
2. Make a connection between trauma & current feelings
3. Encourage - verbalization
- adaptive coping strategy
- exercise
- relaxation technique
4. Provide a quiet, non-stimulating environment to promote sleep
5. Facilitate progressive review of trauma & consequences
6. Suicide contract
7. SOMATOFORM DISORDER
Presence of physical symptoms
These symptoms are real symptoms as experienced by the client
These symptoms are not under the client's conscious control
Laboratory exams would reveal negative results which means that there is no physiologic basis
CAUSE: Anxiety
Secondary Gain
GOAL OF NSG CARE: Reduce ANXIETY? Encourage verbalization!
TYPES:
1. SOMATIZATION: several, multiple somatic complaint
4 PAIN/2 GIT/1 SEXUAL/1 PSEUDONEUROLOGIC
2. CONVERSION: sudden deficit in motor or sensory function. Often these symptoms are exaggerated.
3. PAIN: frequent complaints of pain unrelieved by analgesics severe enough to seek treatment.
4. HYPOCHONDRIASIS: presence of DISEASE CONVICTION & DISEASE PHOBIA. Preoccupation with symptoms.
5. BODY DYSMORPHIC: preoccupations with deficits in physical appearance.
SOMATOFORM RELATED DISORDERS (FACTITIOUS DISORDER)
Presence of symptoms which are under the client's conscious control
CAUSE: Secondary Gain
1. INCENTIVES: Malingering
2. ATTENTION (symptoms are inflicted to self) - MANCHAUSSEN SYNDROME
(symptoms are inflicted to others) - MANCHAUSSEN BY PROXY
MGT: Limit secondary gain
Characterized by at least 6 months of persistent & excessive worry & anxiety
Most common anxiety disorder
Presence of 3 or more of the following evidences of anxiety:
- restlessness
- fatigue
- irritability
- decrease ability to concentrate
- muscle tension
- disturbed sleep
1. Reduce anxiety: develop trust, promote acceptance & convey empathy
encourage verbalization
2. Assist patient in examining problem solving methods
- Discuss present & previous coping mechanism
- discuss meaning of problem & coping
- explore alternate solutions & behaviors
- test new adaptive coping behavior
- relaxation exercises & recreational activities
2. Panic Disorder
recurrent panic attacks & are worried about having more attacks
fear of losing control, feeling of going crazy, having heart attacks, and or dying
associated with agoraphobia
DURATION: 30 minutes to 1 Hour PEAK: 10 minutes
NSG CARE:
1. Promotes safety measures & comfort
- provide a quiet, non stimulating environment
- ensure privacy
- stay with the client
3. Provide relaxation exercises
4. Engage client to explore how to lessen stressors & anxiety provoking situations
3. Obsessive-Compulsive Disorder
OBSESSION: refers to the recurrent & persistent thoughts/ideas/impulses COMPULSION: refers to the repetitive & ritualistic actions/behavior
ergo when we say OBSESSIVE-COMPULSIVE disorder the client is having a persistent & recurrent thoughts/impulse that consumes the person therefore leading to anxiety. In order for the client to neutralize the anxiety the client has to do things over and over again that interferes with the clients activities of daily living.
NSG CARE:
1. Encourage the client to talk about feelings/obsessions/rituals
2. Gradually lessen the time for the client to carry out ritualistic behavior
3. Encourage the client to use techniques to manage anxiety
4. Assist client to complete daily routine & activities
4. PHOBIC DISORDER
intense irrational fear of an external object, activity or situations.
- AGORAPHOBIA: fear of being in a public place
- SOCIAL PHOBIA: fear of being humiliated, scrutinized, or embarrassed in public
- SPECIFIC PHOBIA: fear of a specific object/situation
NSG CARE:
1. Non-critical attitude
2. Provide safety & comfort measures
3. Help patient recognize that their behavior is a method of avoiding anxiety
4. Behavior Therapy
- Systematic Desensitization. Progressive exposure to the feared object in a safe setting until the client's anxiety decreases.
- FLOODING. Rapid exposure with the phobic object until it no longer produces anxiety.
5. DISSOCIATIVE DISORDER
group of mental disorder that affects a client's consciousness, memory, identity, or environmental perception.
DEFENSE MECHANISM: DISSOCIATION. Helps a person protect the emotional self from recognizing the full effect of a traumatic event by allowing the mind to forget or remove itself from the painful memory.
TRAUMATIC EVENT --> FEAR/HORROR --> DISSOCIATIOVE SYMPTOMS (DURING/IMMEDIATELY AFTER EVENT)
DISSOCIATIVE AMNESIA: Loss of memory
DISSOCIATIVE FUGUE: Escape!
DEPERSONALIZATION: Client is detach from mental process or body
DISSOCIATIVE IDENTITY D/O: 2 or more distinct identities that
recurrently take control of behavior accompanied by inability to recall
personal information.
NSG CARE:
1. Institute safety measures
2. Establish a therapeutic environment
3. Relaxation technique
4. Use positive distractions: Physical exercise
Music
Talking to others
Recreational activity
5. Promote self-esteem: view client as a survivor of trauma rather than a victim
6. POST-TRAUMATIC STRESS DISORDER
A disorder that develops after an exposure to a clearly identifiable trauma that threatens self, others, & sense of control or hope.
TRAUMATIC EVENT --> FEAR/HORROR --DISSOCIATIVE SYMPTOMS --> FLASHBACK --> SLEEP DIFFICULTY
HYPER VIGILANCE
IRRITABILITY
↓
AVOIDANCE OF STIMULI R/T TRAUMA
↓
IMPAIRMENT IN FUNCTIONING
ONSET: ACUTE within 6 months after event
DELAYED 6 months & more
DURATION: ACUTE 1-3 months
CHRONIC 3 months & more
GOAL OF NSG CARE: Develop TRUST
1. Non-judgmental & honest
2. Make a connection between trauma & current feelings
3. Encourage - verbalization
- adaptive coping strategy
- exercise
- relaxation technique
4. Provide a quiet, non-stimulating environment to promote sleep
5. Facilitate progressive review of trauma & consequences
6. Suicide contract
7. SOMATOFORM DISORDER
Presence of physical symptoms
These symptoms are real symptoms as experienced by the client
These symptoms are not under the client's conscious control
Laboratory exams would reveal negative results which means that there is no physiologic basis
CAUSE: Anxiety
Secondary Gain
GOAL OF NSG CARE: Reduce ANXIETY? Encourage verbalization!
- ACUTE STAGE: alleviate physical symptoms
- remove client in a stressful environment
- Do not challenge or belittle & do not ignore somatic complaints: Matter of fact/caring approach
- Relaxation technique
TYPES:
1. SOMATIZATION: several, multiple somatic complaint
4 PAIN/2 GIT/1 SEXUAL/1 PSEUDONEUROLOGIC
2. CONVERSION: sudden deficit in motor or sensory function. Often these symptoms are exaggerated.
3. PAIN: frequent complaints of pain unrelieved by analgesics severe enough to seek treatment.
4. HYPOCHONDRIASIS: presence of DISEASE CONVICTION & DISEASE PHOBIA. Preoccupation with symptoms.
5. BODY DYSMORPHIC: preoccupations with deficits in physical appearance.
SOMATOFORM RELATED DISORDERS (FACTITIOUS DISORDER)
Presence of symptoms which are under the client's conscious control
CAUSE: Secondary Gain
1. INCENTIVES: Malingering
2. ATTENTION (symptoms are inflicted to self) - MANCHAUSSEN SYNDROME
(symptoms are inflicted to others) - MANCHAUSSEN BY PROXY
MGT: Limit secondary gain
PERSONALITY DISORDERS
Extreme, rigid, maladaptive & inflexible personality trait. Persons with PD would have deviation on the following area:
1. Cognition
2. Affect
3. Interpersonal Functioning
4. Impulse Control
CLUSTER A PERSONALITY DISORDERS: Odd, Eccentric Behavior
1. PARANOID P.D.
Suspicious & mistrustful of others
Guarded & hypervigilant
Lability in mood from quietly observing to angry outburst
Uses projection as defense mechanism
NSG CARE:
1. Serious, straightforward approach: No joke
No social chit-chat
2. Develop TRUST- Be consistent in keeping appointments
3. Assume a neutral position- must keep an open posture
4. Teach client to validate ideas first before acting
5. Involve client in treatment planning
2. SCHIZOID P.D.
Aloof & indifferent
Socially withdrawn
Highly intellectual i.e. more on solving puzzles and doing mathematical operations
Preoccupied with things rather than interacting with people
NSG CARE:
1. Develop sense of belongingness
2. Initiate interaction: One-on-one interaction
Group interaction
If client entered group interaction, what role can the client assume? MEMBER.
3. Improve functioning in the community: Social Skills Training
3. SCHIZOTYPAL P.D.
Acute discomfort during social gathering
Has no capacity to develop a closed relationship
Pre-morbid personality of clients with schizophrenia: ODD appearance
ODD beliefs
NSG CARE:
1. Direct, professional approach
2. Odd beliefs are simply accepted.
3. Respect client's need for space.
4. Avoid over-involvement
5. Solitary activities
6. Social skills training focused on Hygiene & Grooming
Suspicious & mistrustful of others
Guarded & hypervigilant
Lability in mood from quietly observing to angry outburst
Uses projection as defense mechanism
NSG CARE:
1. Serious, straightforward approach: No joke
No social chit-chat
2. Develop TRUST- Be consistent in keeping appointments
3. Assume a neutral position- must keep an open posture
4. Teach client to validate ideas first before acting
5. Involve client in treatment planning
2. SCHIZOID P.D.
Aloof & indifferent
Socially withdrawn
Highly intellectual i.e. more on solving puzzles and doing mathematical operations
Preoccupied with things rather than interacting with people
NSG CARE:
1. Develop sense of belongingness
2. Initiate interaction: One-on-one interaction
Group interaction
If client entered group interaction, what role can the client assume? MEMBER.
3. Improve functioning in the community: Social Skills Training
3. SCHIZOTYPAL P.D.
Acute discomfort during social gathering
Has no capacity to develop a closed relationship
Pre-morbid personality of clients with schizophrenia: ODD appearance
ODD beliefs
NSG CARE:
1. Direct, professional approach
2. Odd beliefs are simply accepted.
3. Respect client's need for space.
4. Avoid over-involvement
5. Solitary activities
6. Social skills training focused on Hygiene & Grooming
CLUSTER B PERSONALITY DISORDERS: dramatic & emotional
1. ANTI-SOCIAL P.D.
Over-developed ID, disturbed EGO, underdeveloped SE
Manipulative
NSG CARE:
1. Firmness and consistency
2. Supportive confrontation: Neutral
Matter-of-fact approach
2. BORDERLINE P.D.
Lability in mood
Self-destructive behavior (IMPULSIVE)
Strong-dependency need (FEAR OF ABANDONMENT whether real or unreal)
GOAL OF NSG CARE: Discuss feelings rather than to act out impulses
1. Ensure SAFETY- institute SUICIDE PRECAUTION
2. Establish a THERAPEUTIC ENVIRONMENT: offer oneself
active listening
empathetic understanding
3. Establish boundary: use of journal
3. HISTRIONIC P.D.
Attention-seeker: creates scenarios
sexually provocative
NSG CARE:
1. Consistency & limit setting
2. Provide feedback
3. Active listening
4. Respecting personal provocations
4. NARCISSISTIC P.D.
Clients with high self-esteem
Regards self as SPECIAL & UNIQUE
Grandiosity (Self-conceited)
Sense of entitlement
Arrogant
NSG CARE:
1. Help client focus on identification & expression of feelings
2. Supportive confrontation: Neutral
Matter-of-fact
3. Limit setting
Over-developed ID, disturbed EGO, underdeveloped SE
Manipulative
NSG CARE:
1. Firmness and consistency
2. Supportive confrontation: Neutral
Matter-of-fact approach
2. BORDERLINE P.D.
Lability in mood
Self-destructive behavior (IMPULSIVE)
Strong-dependency need (FEAR OF ABANDONMENT whether real or unreal)
GOAL OF NSG CARE: Discuss feelings rather than to act out impulses
1. Ensure SAFETY- institute SUICIDE PRECAUTION
2. Establish a THERAPEUTIC ENVIRONMENT: offer oneself
active listening
empathetic understanding
3. Establish boundary: use of journal
3. HISTRIONIC P.D.
Attention-seeker: creates scenarios
sexually provocative
NSG CARE:
1. Consistency & limit setting
2. Provide feedback
3. Active listening
4. Respecting personal provocations
4. NARCISSISTIC P.D.
Clients with high self-esteem
Regards self as SPECIAL & UNIQUE
Grandiosity (Self-conceited)
Sense of entitlement
Arrogant
NSG CARE:
1. Help client focus on identification & expression of feelings
2. Supportive confrontation: Neutral
Matter-of-fact
3. Limit setting
CLUSTER C PERSONALITY DISORDER: anxious & fearful
1. AVOIDANT P.D.
Viewed self as inferior & unappealing
highly sensitive to criticism
NSG CARE:
1. Provide support & reassurance
2. Assertiveness training
3. Social skills training
4. Gradual immersion to group
2. DEPENDENT P.D.
Submissive & clingy
Strong dependency need: FEAR OF SEPARATION
Inability to make decision
NSG CARE:
1. Foster autonomy & self-reliance
2. Assistance in daily functioning
3. OBSESSIVE-COMPULSIVE
Preoccupation with details
Ability to complete task compropmised by PERFECTIONISM
Reluctant to delegate task
NSG CARE:
1. Explore feelings
2. Assist in task-completion
3. Teach the importance of leisure
Viewed self as inferior & unappealing
highly sensitive to criticism
NSG CARE:
1. Provide support & reassurance
2. Assertiveness training
3. Social skills training
4. Gradual immersion to group
2. DEPENDENT P.D.
Submissive & clingy
Strong dependency need: FEAR OF SEPARATION
Inability to make decision
NSG CARE:
1. Foster autonomy & self-reliance
2. Assistance in daily functioning
3. OBSESSIVE-COMPULSIVE
Preoccupation with details
Ability to complete task compropmised by PERFECTIONISM
Reluctant to delegate task
NSG CARE:
1. Explore feelings
2. Assist in task-completion
3. Teach the importance of leisure
SUBSTANCE ABUSE
Is considered to be a FAMILY DISORDER.
CODEPENDENCY- Maladaptive behavior on the part of the family
CODEPENDENCY- Maladaptive behavior on the part of the family
SUBSTANCE ABUSE
Use of substance inconsistent with medical purpose
Use of substance leads to a negative effect on the client
Use of substance leads to a negative effect on the client
SUBSTANCE DEPENDENCE
Maladaptive use of substance as manifested by:
TOLERANCE- an increased amount of substance is needed to achieve desired result.
WITHDRAWAL- a negative body reaction occur when the client suddenly stops the use of substance
TOLERANCE- an increased amount of substance is needed to achieve desired result.
WITHDRAWAL- a negative body reaction occur when the client suddenly stops the use of substance
SUBSTANCE ABUSER
Anxiety
Low self-esteem
Ineffective coping mechanism
Low self-esteem
Ineffective coping mechanism
DEFENSE MECHANISM
1. Denial
2. Rationalization
3. Projection
2. Rationalization
3. Projection
GOAL OF NSG CARE: Abstinence
1. Reduce substance abuse: provide health teaching
** Lifestyle modification occurs when a person becomes AWARE!
2. Improve clients functioning in the community- engage client in productive activities
3. Address CODEPEnDENCY
** Lifestyle modification occurs when a person becomes AWARE!
2. Improve clients functioning in the community- engage client in productive activities
3. Address CODEPEnDENCY
ALCOHOL (ETHANOL)
Is a primary drug problem
Commonly abused substance
CNS depressant rapidly absorbed in the bloodstream.
ALCOHOL INTOXICATION
Alcohol consumption above alcohol tolerance
Lack of coordination
Attention/concentration is impaired
Blackout
Impaired judgment
Slurred speech
INDICATOR: Breath Odor
CONFIRMATORY: Blood Alcohol Level (0.08 - 0.1% or 80-100 mg/dL blood)
MGT: REST
ALCOHOLISM
Chronic use of alcohol
Alcohol consumption above customary use that interferes with ADL.
ALCOHOLIC FEATURE:
Tolerance
Loss of control
Craving
Physical dependence
LONG-TERM EFFECTS OF ALCOHOL USE
1. Liver Damage
2. Wernicke's Korsakoff Syndrome- due to THIAMINE DEFICIENCY
Commonly abused substance
CNS depressant rapidly absorbed in the bloodstream.
ALCOHOL INTOXICATION
Alcohol consumption above alcohol tolerance
Lack of coordination
Attention/concentration is impaired
Blackout
Impaired judgment
Slurred speech
INDICATOR: Breath Odor
CONFIRMATORY: Blood Alcohol Level (0.08 - 0.1% or 80-100 mg/dL blood)
MGT: REST
ALCOHOLISM
Chronic use of alcohol
Alcohol consumption above customary use that interferes with ADL.
ALCOHOLIC FEATURE:
Tolerance
Loss of control
Craving
Physical dependence
LONG-TERM EFFECTS OF ALCOHOL USE
1. Liver Damage
2. Wernicke's Korsakoff Syndrome- due to THIAMINE DEFICIENCY
WERNICKE'S ENCEPHALOPATHY
acute stage of THIAMINE DEFICIENCY
Double vision
Involuntary & rapid eye movement
Lack of coordination
Memory Deficit
Double vision
Involuntary & rapid eye movement
Lack of coordination
Memory Deficit
KORSAKOFF SYNDROME
Chronic stage of THIAMINE DEFICIENCY
Confusion
Anterograde Amnesia
Retrograde Amnesia
Ataxia
Confusion
Anterograde Amnesia
Retrograde Amnesia
Ataxia
NSG CARE:
1. Remove all sources of alcohol
2. Provide a SAFE ENVIRONMENT: Stay with the client
Do not drive
Remove all harmful objects
3. Establish a therapeutic environment: Develop TRUST
Address A-L-I
ANXIETY- Active Listening
LOW SELF ESTEEM- Activity that ensures success
INEFFECTIVE COPING MECHANISM- Promote coping mechanism
4. Provide supplements- Thiamine & B-Vitamins
5. Group Therapy: Alcoholic Anonymous
Alanon
Alateen
6. Aversion Therapy- to deter client fromdrinking
DOC- ANTABUSE(DISULFIRAM)
FOCUS: No alcohol 12 hours before & 14 days after
INSTRUCTIONS: Read label
Avoid alcohol: Cough Syrup
Lotion
Aftershave
Mouthwash
Perfume
ALCOHOL WITHDRAWAL
Seizure
Hallucination
Increased v/s (BP & PR) & increased sweating
Tremors
**SH--> Delirium Tremens (occurs within 48-72 Hours)
**IT--> Early Signs
DOC: BENZODIAZEPINES: Lorazepam (Ativan)
Chlordiazepoxide (Librium)
Diazepam (Valium)
2. Provide a SAFE ENVIRONMENT: Stay with the client
Do not drive
Remove all harmful objects
3. Establish a therapeutic environment: Develop TRUST
Address A-L-I
ANXIETY- Active Listening
LOW SELF ESTEEM- Activity that ensures success
INEFFECTIVE COPING MECHANISM- Promote coping mechanism
4. Provide supplements- Thiamine & B-Vitamins
5. Group Therapy: Alcoholic Anonymous
Alanon
Alateen
6. Aversion Therapy- to deter client fromdrinking
DOC- ANTABUSE(DISULFIRAM)
FOCUS: No alcohol 12 hours before & 14 days after
INSTRUCTIONS: Read label
Avoid alcohol: Cough Syrup
Lotion
Aftershave
Mouthwash
Perfume
ALCOHOL WITHDRAWAL
Seizure
Hallucination
Increased v/s (BP & PR) & increased sweating
Tremors
**SH--> Delirium Tremens (occurs within 48-72 Hours)
**IT--> Early Signs
DOC: BENZODIAZEPINES: Lorazepam (Ativan)
Chlordiazepoxide (Librium)
Diazepam (Valium)
